

Mental health in elite athletes: International Olympic Committee consensus statement
Elite athletes often experience mental health symptoms and disorders, which can have sport-related manifestations and impair performance. Physical and mental health are inextricably linked, as mental health disorders can increase the risk of injury and delay physical injury recovery. According to established guidelines, the symptoms and conditions of mental health in elite athletes are not well documented or treated. Elite athletes must be differentiated from individuals with psychosocial maladaptations in diagnosis. To minimize adverse effects on athletes, management strategies should address the wide range of factors contributing to their mental health symptoms. To optimize the performance of all elite athletes, sports management must include both treatments for individual athletes and optimizing the training and competition environment. As part of the International Olympic Committee’s Consensus Work Group aimed at advancing the adoption of a more standardized and evidence-driven approach to mental health symptoms and disorders among elite athletes, critically reviewed current scientific findings and recommendations were made.
At a consensus meeting convened by the International Olympic Committee (IOC) in Lausanne, Switzerland, on 12-14 November 2018, experts examined the scientific literature regarding mental health symptoms and disorders in athletes. Participants analyzed the best evidence and drafted recommendations for clinical practice and individual and systemic interventions to improve mental health among elite athletes. Professional athletes, Olympic athletes, and collegiate athletes are considered elite. In this paper, we include college and professional athletes since the training and competition levels are similar.
Tasks assigned to the group included:
- to review mental health symptoms and disorders in elite athletes: prevalence, diagnosis, and impact on athletic performance
- to review the literature and to establish guidelines regarding non-pharmacological and pharmacological treatment of mental illness in athletes;
- to provide recommendations on minimizing negative impacts of the sports environment on mental health symptoms and disorders in elite athletes.
Using different models and perspectives, this consensus document addresses mental health symptoms among elite athletes in fulfilling the IOC charge. It is aimed at practitioners in sporting medicine and other clinicians (including physiotherapists and athletic trainers) and psychiatrists and other licensed mental health professionals, as well as researchers in the field of elite athlete mental health, and clinical or institutional leaders and administrators in sport.
Methods
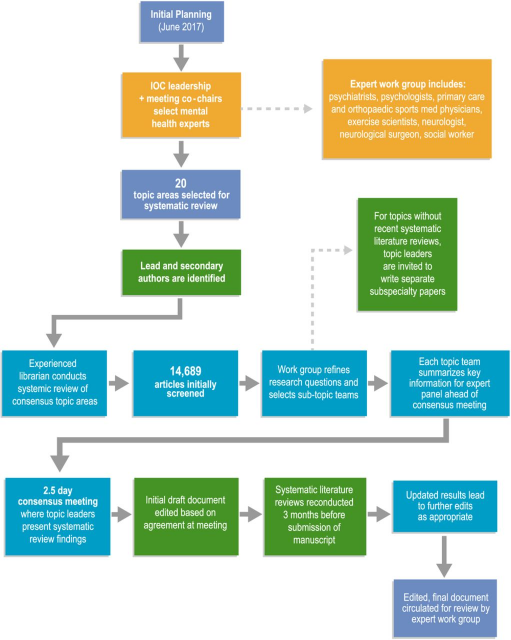
Several months before the consensus meeting took place (figure 1), preparations were begun. As initially organized, both the meeting (CLR and BH) co-chairs and the IOC leadership (RB and LE) took part in the process. Experts from 13 nations were identified to form a panel of 23 individuals who provide expertise in the mental health of elite athletes. Over the past five years, an evaluation of their publications was used to identify panelists based on specific topics of mental health symptoms and disorders in elite athletes and invite them based on their clinical/scientific knowledge of these topics. A working group was formed with the experts invited, the organizers, four medical and scientific experts, and two representatives from the elite athletes. Invitation to one expert panelist failed to receive a response, so he was omitted, and another was eliminated due to inactivity after initially being included. The final workgroup was comprised of a neurologist, a neurosurgeon, an exercise scientist, a psychiatrist, a psychologist, and a social worker.
Systematic Reviews
The following sections describe how a meeting was planned and prepared, how it was conducted, and how the consensus statement was written. To generate a consensus statement, the organizing group identified 20 topic areas (Figure 1). With scientific expertise and clinical expertise, an author (or authors) was assigned to each study as the lead author and sometimes as a secondary author. A librarian conducted systematic reviews of each topic area using databases such as PubMed, SportDiscus, PsycINFO, Scopus, Cochrane, and other databases relevant to each topic by area leaders. Study designs of all types were included in the search, and only English was used in the search. An initial search strategy was developed with input from the expert panel to capture all relevant search terms. The librarian revised searches as needed. The expert panel screened 14689 published articles. A revised set of 20 research topic areas was developed based on the results and input of the expert panel. Due to the lack of a recently published systematic review, leading authorities were invited to write more detailed papers on their subject areas; these papers will be published separately. In the final step, the topic teams must summarize their key findings and present them to the expert panel before the consensus meeting. Before the meeting, a draft of these summaries was circulated to all participants. Topic leaders presented their systematic review findings at the consensus meeting, which lasted 2.5 days. A group discussion followed each presentation, and meeting co-chairs recorded each comment.
Drafting the consensus statement
Based on the agreement at the meeting, the initial draft of the systematic review summary document was edited. During the drafting of the final document, key points agreed upon during the meeting were not changed. They Re-conducted the systematic literature reviews three months before the manuscript was submitted, using the same search strategies as originally employed. Topic leaders received updated search results, and edits were made accordingly. The finalized version of the edited manuscript was circulated to the full panel of expert reviewers for further editing.
THE COMPLETE ARTICLE CAN BE READ AT THIS LINK
Directions for the future
Based on the current state of knowledge and the current state of science in mental health in elite athletes, future research, changes in clinical practice, and environmental optimization are possible directions for future research. Included are:
1. There are several countries and cultures where mental health services are not available, and this must be considered when developing clinical services and research. Mental healthcare should be based on rigorous evidence in every country. The provision of that care may call for a more nuanced approach, including athletes’ physical and occupational therapists, coaches, and anyone in the athlete’s entourage or community in the mental healthcare team. Researchers and practitioners must use existing evidence and lessons from global mental health if elite athletes are to receive equitably available mental healthcare.
2. A more thorough and reliable study of the prevalence of mental health disorders in elite athletes is necessary, one that considers cross-cultural differences in mental health disorders. A lack of data is particularly evident in mental health emergencies, bipolar disorders, and athletes with disabilities.
3. More robust research is needed on the effects of subconcussive impacts on mental health, such as pre-existing mental health conditions as risk factors.
4. Research on athlete symptoms should distinguish them from full disorders; athletes with symptoms themselves can pose a problem for elite athletes, and therefore should remain a focus of research. In addition, early symptomatic stages of full disorders need to be clarified within elite athletes to increase understanding of risk factors.
5. Expansion of mental health screening for elite athletes needs further study and subsequent recommendations. The goal of screening is to ensure better that affected elite athletes eventually receive the care they need. There is a need for careful consideration in the timing of screening, given that risks, such as those associated with injury, increase throughout an elite athlete’s career. Sports-specific screening tools may be beneficial in several diagnostic categories that do not yet have them, considering the unique manifestations of these conditions in this population while also appreciating the limitations of relying solely on rating scales without clinical interviews. Understanding the unique symptoms manifested in athletes may require qualitative and quantitative research across cultures and countries to develop optimal assessment methodologies.
6. Playing again after an injury or illness requires a better understanding of the physiological recovery process and the optimum readiness to return to play. In this context, one must consider the impact of sleep on recovery and readiness.
7. Psychotherapy and pharmaceutical treatment for mental health problems encountered by elite athletes require more research. Pharmacologic research should include addressing the limitations that have been identified so far. For example, some countries and cultures use therapies and medications/supplements disproportionately than others, but there may be a lack of evidence supporting these practices. In addition, additional research is needed regarding medications to treat mental health symptoms associated with concussions such as depression and anxiety.
8. Existing mental health prevention strategies need to be improved. For example, an eating disorder and substance abuse disorder prevention plan, especially within high-risk elite sports, is necessary. It would also be helpful if elite sport prevention strategies were more widely implemented.
9. Elite athlete populations must be protected from stigma in more effective ways so that these individuals come to understand that mental toughness is compatible with mental health help-seeking.
10. Sport as a subculture within society should be better understood, specifically which elements are particularly beneficial to mental health. It is important to continue exploring the developmental factors that can lead to a favorable adjustment in elite sport for members of the athlete entourage, including parents and other caregivers. Treatment effective in alleviating mental well-being must distinguish from actual mental health symptoms.
11. Sleep hygiene should be a priority when designing and assessing Olympic villages and similar areas.
12. Specifically, researchers need to explore how sports sponsorships by companies that promote alcohol, tobacco, and other products can adversely affect elite athletes’ mental health.
13. Mental wellness and mental health help-seeking should be promoted by empowering coaches and athletes with relevant information.
Summary
To reduce suffering and improve the quality of life in elite athletes and serve as a model for society, the IOC has committed to improving mental health among athletes. In the coming years, the IOC hopes all stakeholders will recognize mental health symptoms and disorders treated equally to other medical illnesses and musculoskeletal injury; all can be severe and disabling, and most can be managed with the appropriate medical care. Athletes’ physical and mental health are interconnected and cannot be separated. Athletes should have access to the best interdisciplinary care for their cognitive health as they do for their other medical needs. It has been established that the IOC Consensus Group has taken a critical look at current state-of-the-art research and practice of mental health among elite athletes to advance a more unified and evidence-based approach.
For complete consensus statement follow this link.
Reference:
Reardon, Claudia & Hainline, Brian & Aron, Cindy & Baron, David & Mcduff, David & Baum, Antonia & Bindra, Abhinav & Budgett, Richard & Campriani, Niccolo & Castaldelli-Maia, João & Currie, Alan & Derevensky, Jeffrey & Glick, Ira & Gorczynski, Paul & Gouttebarge, Vincent & Grandner, Michael & Han, Doug & Rice, Simon. (2019). Mental health in elite athletes: International Olympic Committee consensus statement (2019). British Journal of Sports Medicine. 53. 10.1136/bjsports-2019-100715.